|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
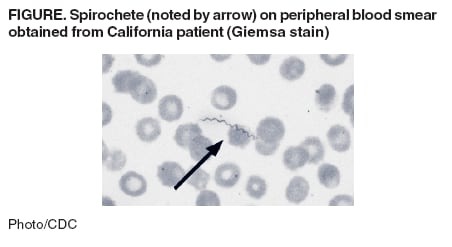
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Acute Respiratory Distress Syndrome in Persons with Tickborne Relapsing Fever --- Three States, 2004--2005Tickborne relapsing fever (TBRF) is a bacterial illness caused by certain species of Borrelia and transmitted through brief and painless bites from Ornithodoros ticks (1,2). Illness usually is characterized by intermittent periods of fever, fatigue, and muscle aches. In April 2005, CDC received reports of two cases of severe TBRF associated with acute respiratory distress syndrome (ARDS) in residents of California and Nevada. After a report describing these cases was posted on CDC's Epidemic Information Exchange (Epi-X), health officials in Washington reported a third severe case associated with ARDS. This report summarizes these three cases and the results of the subsequent epidemiologic investigations. The findings indicate that ARDS might occur more frequently in patients with TBRF than previously recognized. Optimal management of TBRF requires both prompt diagnosis and careful observation during the initial phases of treatment. Case ReportsNevada. On February 17, 2005, a previously healthy woman aged 46 years from Washoe County, Nevada, had onset of nonspecific leg pain, which progressed during the next 24 hours to generalized myalgia. She visited a local hospital emergency department (ED), where a viral syndrome was diagnosed. She was treated with intravenous (IV) fluids and pain medication and discharged home. Two days later, she returned to the ED with fever, chills, fatigue, anorexia, nausea, and an episode of syncope. On arrival, she was noted to be tachycardic (130 beats per minute [bpm]), tachypneic (24 breaths per minute), and hypotensive (systolic blood pressure: 89 mm Hg) with a temperature of 96.8°F (36.0°C). A physical examination was otherwise unremarkable. Pulse oximetry on room air indicated an oxygen saturation of 96%. Initial laboratory testing revealed a white blood cell count (WBC) of 11.4 × 103/µL, hemoglobin level of 13 g/dL, platelet count of 66 × 103/µL, and alanine aminotransferase (ALT) of 153 U/L. A chest radiograph revealed a right middle lobe infiltrate, consistent with community-acquired pneumonia. She was treated with gatifloxacin and transferred to the intensive care unit (ICU). Approximately 10 hours after admission, she was intubated for worsening tachypnea (respiratory rate [RR]: 40 breaths per minute). Diffuse bilateral infiltrates were noted on chest radiograph, and an arterial blood gas sample yielded oxygenation of 53 mmHg on 100% inspired oxygen. The patient's antimicrobial treatment was broadened to include vancomycin and doxycycline. The next day, the treating physician was notified that spirochetes were observed during examination of a blood smear obtained when the patient was admitted; the smear had been manually reviewed because of thrombocytopenia. The patient remained intubated for 12 days for what was ultimately determined to be ARDS. During this time, she was administered three additional antimicrobials (ciprofloxacin, tobramycin, and ceftriaxone) and drotrecogin-a.* She was discharged after 21 days and recovered completely. The causative organism was identified as Borrelia hermsii by polymerase chain reaction (PCR) performed on a whole blood sample and serologic testing of convalescent-phase serum, both performed at CDC. Although the patient did not recall receiving a tick bite, she did report staying at a resort near South Lake Tahoe (an area known to be highly endemic for TBRF) 5 days before becoming ill. California. On April 12, 2005, a previously healthy woman aged 43 years from El Dorado County, California, had onset of lethargy and myalgia. She went to a local hospital ED on April 14 with fever, chills, headache, myalgia, and dehydration. She was febrile (100.5°F [38.1°C]), tachycardic (138 bpm), mildly tachypneic (16 breaths per minute), and hypotensive (systolic blood pressure: 97 mm Hg). A physical examination was otherwise unremarkable. Pulse oximetry on room air indicated an oxygen saturation of 97%. A chest radiograph was not obtained, but initial blood tests indicated an elevated bilirubin level of 3.6 mg/dL, aspartate aminotransferase (AST) of 93 U/L, and ALT of 88 U/L. She was treated with acetaminophen and discharged home with instructions to return for reevaluation of blood tests the next day. The patient returned the next day with headache, sweating, fatigue, and nausea. A physical examination revealed rhonchi; a chest radiograph was obtained and read as normal. She was treated with IV fluids and IV ceftriaxone. Within 1 hour of receiving antibiotics, her pulse increased to 127 bpm, her systolic blood pressure decreased to 85 mm Hg, and pulse oximetry on room air indicated an oxygen saturation of 95%. TBRF was diagnosed by observation of spirochetes in smears of peripheral blood (Figure). The patient was treated with dopamine for hypotension and doxycycline for TBRF and transferred to another medical center. Shortly after arrival, a chest radiograph taken because of worsening respiratory distress demonstrated diffuse bilateral infiltrates. The patient was intubated for respiratory failure (RR: 44 breaths per minute; oxygen saturation of 82% on 100% inspired oxygen via nonrebreather mask) attributed to ARDS. Laboratory testing revealed a WBC of 3.4 × 103/µL, hemoglobin level of 11.4 g/dL, and platelet count of 19 × 103/µL. Platelets and fresh frozen plasma were administered. The patient remained intubated for 10 days, during which she was administered four different antimicrobials (vancomycin, piperacillin/tazobactam, metronidazole, and doxycycline) and drotrecogin-a. She was discharged after 19 days of hospitalization and eventually recovered from her illness. A blood sample obtained early in illness and cultured at CDC yielded B. hermsii. An environmental investigation was conducted at her home, located 5 miles south of Lake Tahoe and approximately 10 miles from the resort visited by the Nevada patient. An engorged soft tick was found in her bedroom, and removal of house siding revealed multiple rodent nests from which approximately 30 Ornithodoros hermsi ticks were recovered. Washington. A woman aged 40 years from King County, Washington, visited a hospital ED on September 21, 2004, with myalgia, arthralgia, nausea, vomiting, and headache. She was treated with IV fluids, promethazine, and hydrocodone. Hospital admission was recommended, but she refused. After experiencing a syncopal episode at home, she returned and was noted to be febrile (102ºF [38.9°C]), hypotensive (systolic blood pressure: 100 mm Hg), mildly tachycardic (107 bpm), and hypoxic (oxygen saturation: 92% on 4 L of oxygen). A physical examination was otherwise unremarkable. Her chest radiograph revealed bilateral lower lobe infiltrates. Initial laboratory studies indicated a WBC of 9.5 x 103/µL, hematocrit of 33%, platelet count of 49 x 103/µL, ALT of 192 U/L, and a D-dimer of 754. She was admitted for presumed community-acquired pneumonia with sepsis and treated empirically with IV cefuroxime and azithromycin. After receiving the cefuroxime, she was transiently hypotensive and became somnolent. She was intubated and transferred to the ICU with a diagnosis of ARDS and worsening mental status. Because of thrombocytopenia, a peripheral blood smear was examined, revealing spirochetes diagnostic of TBRF. Her transient hypotension was attributed to a Jarisch-Herxheimer reaction (JHR).† She remained intubated for 3 days, was discharged home after 10 days, and eventually recovered from her illness. The most likely site of exposure was a forest cabin in Chelan County, Washington, where she had slept approximately 11 days before illness onset. On inspection, the cabin had evidence of rodent infestation; however, attempts to trap ticks and rodents were unsuccessful. Epidemiologic InvestigationsTo determine the frequency of ARDS among patients with TBRF acquired in the South Lake Tahoe area, case-report forms for all TBRF cases reported to Nevada and California state and local health departments during 1995--2004 were reviewed. Additionally, cases were ascertained by 1) a computerized search of discharge records from Lake Tahoe area hospitals where cases had been diagnosed; 2) interviews with physicians and laboratorians from area hospitals and private practices where cases had been diagnosed; and 3) postings on Epi-X and the Emerging Infections Network. Including the California and Nevada cases described in this report, 65 cases of TBRF among persons who reported living in or visiting the Lake Tahoe area during the usual incubation period of 2--18 days before illness onset were ascertained. Thirty (46%) were in patients who required hospitalization. Detailed clinical information from medical records was available for 38 (58%) patients. Among these 38 patients, 16 (42%) experienced one or more of the following complications: eight (21%), JHR; six (16%), hypoxia; five (13%), elevated liver enzyme levels; three (8%), arrhythmia or myocarditis; two (5%), azotemia; and two (5%), ARDS. TBRF cases in Washington state were similarly reviewed by using all case reports submitted to the state health department during 1996--2005. Including the single case described in this report, 46 TBRF cases were reported in Washington during 1996--2005, of which 37 (80%) were in patients who required hospitalization. Comments on case-report forms indicated that five (13%) patients required care in an ICU, three (6%) had JHR, and three (6%) had ARDS. All three ARDS cases occurred after 2001. Reported by: FK Murphy, MD, S Parker, MD, Sierra Infectious Diseases, Reno; D Stokich, M Murray, Washoe County District Health Dept; V Fogelman, DVM, R Todd, DrPH, Nevada State Health Div. V Huber, El Dorado County Environmental Management Dept; A Tabor, N Deatherage, El Dorado County Public Health Dept; J Tucker, C Fritz, DVM, J Mohle-Boetani, MD, California Dept of Health Svcs. C Skilton, MS, Public Health Seattle--King County, Washington. K Kugeler, MPH, M Schriefer, PhD, P Mead, MD, Div of Vector-Borne Infectious Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases; L Minicucci, DVM, E Sergienko, MD, JE Staples, MD, C Wheeler, MD, EIS officers, CDC. Editorial Note:Although TBRF is not a nationally notifiable disease, it is a reportable condition in 11 western states. Each year, approximately 25 cases are reported to CDC, all among residents of or visitors to western states where the disease is endemic (CDC, unpublished data, 2007). Most cases are caused by B. hermsii, which is transmitted to humans through the bite of O. hermsi ticks (1,2). These ticks typically feed for less than 30 minutes and usually at night; consequently, most patients do not recall being bitten. Rodents are vertebrate reservoirs for the disease, and cabins or homes located at elevations of 2,000--7,000 feet in coniferous forests are common exposure sites. Outbreaks associated with such sites have been reported from Arizona, California, Colorado, Montana, New Mexico, and Washington (3--8). Clinical symptoms of TBRF have included fever, headache, myalgia, chills, and nausea. Without antimicrobial treatment, patients typically experience multiple episodes of febrile illness. Rarely reported complications include uveitis, cranial nerve palsy, myocarditis, splenic rupture, and JHR (1,2). Only one case of TBRF with ARDS has been described previously (9), and this case occurred in a woman who was pregnant and therefore more susceptible to severe TBRF (10). Results of this investigation indicate that ARDS might occur more frequently in patients with TBRF than previously recognized and can occur in persons without predisposing conditions. All cases of TBRF-associated ARDS identified in this review occurred after 2001, but further surveillance will be needed to determine whether the risk for ARDS in TBRF is increasing. Increases might be related to changes in medical practice, use of newer antimicrobials, or possibly the emergence of a more virulent strain. All three cases described in this report occurred in women, but no common medical history (e.g., menopausal status, hormone replacement therapy, or oral contraceptive use) was identified. All three patients had received antimicrobial treatment before onset of ARDS; however, whether they had ARDS as a result of JHR or underlying sepsis could not be determined. The findings in this report are subject to at least two limitations. First, cases were evaluated in only two geographic areas; therefore, results might not be generalizable to the endemic western states. Second, TBRF is not a nationally notifiable disease, and each state has different reporting requirements; therefore, case information is subject to underreporting and ascertainment bias. These methodological differences might have affected the observed rates of hospitalization and classification of ARDS. Health-care professionals should report suspected TBRF cases to local or state health departments, providing a thorough clinical and exposure history and, as appropriate, samples (i.e., serum or whole blood) for diagnostic testing. The observation of spirochetes in a Wright- or Giemsa-stained peripheral blood smear collected during a febrile episode is considered diagnostic of TBRF and is not typical of other spirochetal infections (1). Laboratory diagnosis also can be made by culture, serology, or PCR of serum and blood at certain reference laboratories. TBRF can be prevented by minimizing rodent infestations in homes. Health officials in endemic areas should consider educational measures that increase awareness of potential exposures, demonstrate methods for rodent proofing dwellings, and promote early recognition of cases by health-care professionals (5). These measures are especially important in mountainous resort areas that serve numerous visitors. Acknowledgment This report is based, in part, on contributions by J Young, Div of Vector-Borne Infectious Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases, CDC References
* Drotrecogin-a (Xigris®) primarily is used to treat severe sepsis. The drug is a recombinant form of human activated protein C that has antithrombocytic, antiinflammatory, and profibrinolytic properties. † JHR is an acute exacerbation of symptoms, attributed to decreasing bacterial numbers and a massive cytokine release, which can occur during initial treatment of spirochetal infections (e.g., relapsing fever and syphilis) with an effective antibiotic. Symptoms include hypotension, tachycardia, chills, rigors, diaphoresis, and elevated body temperature (1).
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 10/18/2007 |
|||||||||
|