|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
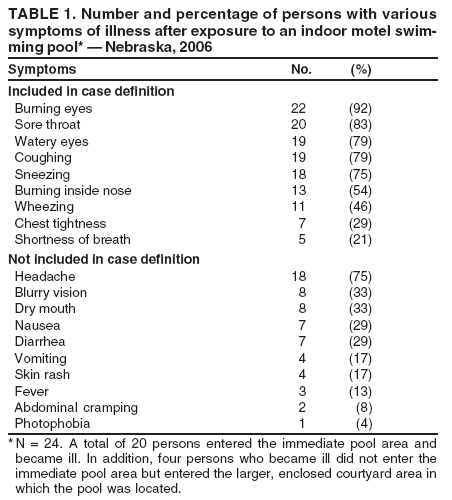
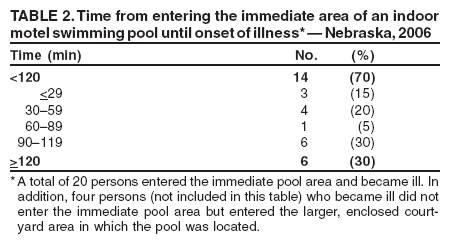
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Ocular and Respiratory Illness Associated with an Indoor Swimming Pool --- Nebraska, 2006On December 26, 2006, the Nebraska Department of Health and Human Services (NDHHS) received a report of a child hospitalized in an intensive care unit for severe chemical epiglottitis and laryngotracheobronchitis after swimming in an indoor motel swimming pool. The pool was inspected the same day and immediately closed by NDHHS because of multiple state health code violations. NDHHS initiated an outbreak investigation to identify additional cases and the cause of the illness. This report describes the results of that investigation, which indicated that 24 persons became ill, and the outbreak likely was the result of exposure to toxic levels of chloramines* (1,2) that had accumulated in the air in the enclosed space above the swimming pool. This outbreak highlights the potential health risks from chemical exposure at improperly maintained pools and the need for properly trained pool operators to maintain water quality. The index patient was an otherwise healthy boy aged 6 years. The boy and his family attended a gathering with relatives at the motel on December 25, 2006, and he spent approximately 3 hours swimming in the pool. During this time, he had onset of coughing and dyspnea. He stopped playing in the pool but continued to cough, with one or two episodes of posttussive emesis. His parents had intended to spend the night at the motel but checked out early and returned to their home (approximately 15 miles away) the evening of December 25. During a period of 5 hours, the boy's condition worsened. He became agitated and more dyspneic and was taken to a local emergency department (ED) with erythematous eyes and nasopharynx, a barking cough, inspiratory stridor, expiratory wheezes, and respiratory distress. The parents told the physician that multiple persons in their group had developed burning eyes, nasal burning, congestion, and cough. Physical examination of the boy indicated croupy cough, stridor at rest, and moderate retractions. Oxygen saturation level was 98% on room air; lungs were clear on auscultation, and no chest radiograph was performed. In the ED, he received a dexamethasone injection, 3 doses of racemic epinephrine, and cool-mist respiratory therapy. He was transferred to the pediatric intensive care unit in stable condition for observation, with a guarded prognosis and a diagnosis of upper airway obstruction from chemical epiglottitis and laryngotracheobronchitis; drug therapy was discontinued, and no additional treatments were administered. The boy's condition gradually improved, and he was discharged the next morning. The attending physician recorded chlorine irritation as the cause of illness. Investigators learned that the motel belonged to a national chain. The indoor, heated pool measured 40 × 32 feet and had a maximum capacity of 70 persons. The immediate pool area was contained within a larger enclosed courtyard area with a single exhaust fan for ventilation in the ceiling directly above the pool. Adjacent guest rooms opened directly into the enclosed courtyard. From the motel registry that recorded the name of a single guest per room, NDHHS identified 110 rooms with at least one guest registered during December 15--26, 2006, and attempted to contact these persons by telephone. Registered guests were asked whether they or other persons in their party experienced illness during their stay. Those who reported illness were asked to complete an online questionnaire; responses from persons without Internet access were collected by telephone. Information was collected regarding basic demographics; exposure to the pool, immediate pool area, or enclosed courtyard; time from exposure to illness onset; symptoms of illness; and whether medical treatment was required. A case was defined as ocular or respiratory illness in a motel guest during December 15--26, with illness onset after arrival and characterized by at least one of the following symptoms: burning eyes, sore throat, watery eyes, coughing, sneezing, burning inside the nose, wheezing, chest tightness, or shortness of breath. NDHHS attempted to contact by telephone all 110 motel guests registered during December 15--26 and reached 67 (61%). Among those persons and other guests staying with them, 24 had illness consistent with the case definition; 16 were male, and eight were female, with a median age of 39 years (range: 4--71 years). In addition to the case definition symptoms, the 24 reported other symptoms (e.g., headache, blurry vision, or dry mouth) (Table 1). Of 24 persons reporting illness, 20 (83%) had entered the immediate pool area, and four (17%) had entered the courtyard only. Among the 20 who entered the immediate pool area, 14 reported exposure for >1 hour, and six reported exposure for 30--60 minutes; 14 (70%) had onset of illness within 2 hours of entering the area (Table 2). Of five persons who sought medical care, three reported swimming in the pool, and two had entered the immediate pool area only. Four of the five persons were children aged <16 years; only the boy aged 6 years (the index patient) was hospitalized. Nebraska health code regulations require clean and clear public swimming-pool water with a clearly visible main drain (3). Acceptable water-chemistry values for swimming pools are as follows: free chlorine, 2--10 ppm; pH, 7.2--7.8; and chloramine (measured as combined chlorine†), <0.5 ppm (3). Inspection of the motel pool on December 26 revealed multiple state health code violations, including cloudy water, a free chlorine level (0.8 ppm) less than half the minimum, a chloramine level (4.2 ppm) eight times the maximum, and a pH (3.95) approximately half the minimum. Less severe violations included low alkalinity, inadequate daily logs, and an inoperable flow meter. Review of operator logs indicated deterioration of the pool's water quality during the weeks preceding the outbreak. Before pool closure, the operator recorded inadequate combined chlorine levels for 26 consecutive days. Each log entry for combined chlorine on these days was at least three times higher than the acceptable limit of 0.5 ppm, ranging from 1.8--7.0 ppm. During this same period, the operator also recorded pH levels below the lowest acceptable limit of 7.2 on 14 of 26 days and free chlorine levels below the lowest acceptable limit of 2.0 ppm on 5 of 26 days. In addition to improper management of the water chemistry, the ceiling exhaust fan was turned off at the time of the outbreak, and the outside windows of the enclosed courtyard were closed because of cold outdoor air temperatures. The pool was closed on December 26 and subsequently drained. It reopened February 7, 2007, and no additional illnesses have been reported. Reported by: T Safranek, MD, S Semerena, MBA, T Huffman, M Theis, Nebraska Dept of Health and Human Svcs. J Magri, MD, T Török, MD, Office of Workforce and Career Development; MJ Beach, PhD, Div of Parasitic Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases; B Buss, DVM, EIS Officer, CDC. Editorial Note:Swimming is the most popular recreational activity among children in the United States and the second most popular exercise activity for all ages, with approximately 360 million visits to recreational water venues each year (4). Throughout the country, swimming-pool operators are responsible for proper maintenance of public pools and receive minimal public health oversight (5). This outbreak in Nebraska highlights the public health risk of improperly managed public pools. Long-term deterioration of the pool water quality was documented by the operator, who failed to maintain acceptable levels set by state regulations. Although NDHHS is responsible for overseeing the training certification of municipal pool operators, Nebraska state regulations do not require training or certification for operators of state-licensed, nonmunicipal public pools; therefore, the operator of this swimming pool was not required to be certified and had no verifiable training. Chloramines can remain in the water or evaporate into the air above the pool, causing a pungent smell. Trichloramine is more volatile than monochloramine and dichloramine and is released into the air more readily. In addition, trichloramine causes more severe irritation and forms more rapidly in water with a low pH, such as the water in this pool (2). Methods to test chloramine levels in the air exist but are neither routine nor rapid. Therefore, environmental air sampling was not performed as part of this outbreak investigation, and the outbreak could not be specifically linked to elevated levels of chloramines in the air. However, several factors strongly suggest that high chloramine levels in the air were the cause of illness. First, the water's combined chlorine level of 4.2 ppm (at least eight times the acceptable level), together with the water's extremely low pH (3.95), was favorable for formation of high levels of chloramines, particularly trichloramine. Second, all 24 ill persons reported that their symptoms began after they entered the pool courtyard environment, and 70% of ill persons who entered the immediate pool area reported illness onset within 2 hours of entering the area. Finally, ventilation was inadequate during the outbreak; the windows of the pool enclosure were closed, and the ceiling exhaust fan had been turned off, presumably to retain a warmer temperature in the enclosed courtyard. Chloramines are not considered health hazards in outdoor swimming pools. However, in the enclosed space around indoor pools, they can reach dangerous concentrations and pose a substantial health risk. High concentrations cause acute eye and respiratory tract irritation in swimmers and other persons in the indoor pool environment (1,2) and might also contribute to asthma and respiratory disease (6,7). In 2004, two similar outbreaks associated with exposure to indoor motel swimming pools were reported in Illinois (8). Within minutes of entering the indoor pool environments, 72 persons, predominantly children, reported illness with high attack rates and symptoms consistent with chloramine exposure. Water-chemistry abnormalities and inadequate pool maintenance were cited as contributing factors; the investigators suggested that standard education be mandatory for all public pool operators (8). The findings of this investigation are subject to at least two limitations. First, NDHHS was unable to reach all 110 registered hotel guests, and those who were contacted were asked to complete an online survey. This passive method of data collection likely reduced the number of respondents, possibly resulting in an underestimation of the extent of the outbreak. Second, the association between exposure and illness could not be quantified because illness was not assessed in persons who were not exposed. Clinicians and public health professionals should be vigilant for outbreaks of illness related to recreational water exposure, including those involving exposure to chloramines; such outbreaks should be reported to health departments. Chloramine-related outbreaks are thought to be common but seldom reported (8,9). Although NDHHS certification for nonmunicipal pool operators is not required, NDHHS training courses are open to both municipal and nonmunicipal pool operators. To ensure the safety of indoor swimming-pool environments, pool owners should ensure that pool operators are trained to maintain water chemistry within acceptable ranges and ensure adequate ventilation to prevent accumulation of unsafe levels of chloramines and minimize the associated health risks. In addition, swimmers should report an unusually strong chlorine odor and any instance of pool-associated respiratory or ocular irritation to pool operators and refrain from entering the implicated pool area and swimming in the pool. References
* Disinfection by-products formed when free chlorine, a common disinfectant used in swimming pools, combines with nitrogenous human wastes (e.g., sweat, urine, or feces) in pool water. † Combined chlorine = total chlorine -- free chlorine.
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 9/12/2007 |
|||||||||
|