 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
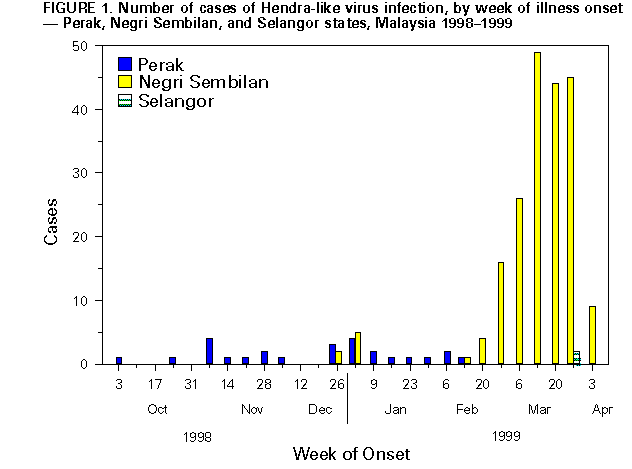
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreak of Hendra-Like Virus -- Malaysia and Singapore, 1998-1999During September 29, 1998-April 4, 1999, 229 cases of febrile encephalitis (111 {48%} fatal) were reported to the Malaysian Ministry of Health (MOH). During March 13-19, 1999, nine cases of similar encephalitic illnesses (one fatal) and two cases of respiratory illness occurred among abattoir workers in Singapore. Tissue culture isolation identified a previously unknown infectious agent from ill patients. This report summarizes the preliminary epidemiologic and laboratory investigations of these cases, which indicate that a previously unrecognized paramyxovirus related to, but distinct from, the Australian Hendra virus is associated with this outbreak. MALAYSIA A case of suspected illness was defined as fever, severe headache, myalgia, and signs of encephalitis or meningitis. Three clusters of cases have been identified. The first cluster began in late September 1998 near the city of Ipoh in the state of Perak. Cases continued to occur in this region until early February 1999. The second cluster occurred near the city of Sikamat in the state of Negri Sembilan in December 1998 and January 1999. The third and largest cluster began near the city of Bukit Pelandok in the state of Negri Sembilan in December 1998. Two cases occurred in the state of Selangor (Figure_1). Cases have occurred primarily among adult men who had histories of close contact with swine. Concurrent with the human cases, illness and death occurred among swine from the same regions. Initially, Japanese encephalitis (JE) virus was considered the probable etiologic agent for this outbreak, and specimens from some patients tested positive for infection with JE virus. However, the predominance of cases in men who had close contact with swine suggested the possibility of another agent. Laboratory Features Tissue culture isolation from central nervous system specimens at the Department of Medical Microbiology, University of Malaya, identified a previously unknown infectious agent. Additional laboratory analysis at CDC of samples from 13 patients found recent JE virus infection in only one of 13 serum specimens. Electron microscopic studies of isolation material from three patients demonstrated virus-like structures consistent with a paramyxovirus, and immunofluorescence tests of cells infected with this virus suggested a virus related to Hendra virus (formerly called equine morbillivirus). Additional laboratory testing, including preliminary nucleotide sequence information, indicated the virus was related but not identical to the Hendra virus. Using a capture-IgM ELISA with prototype Hendra virus antigens, IgM antibodies were detected in the 12 JE-negative serum specimens. Tissues from three of four case-patients who died contained viral antigen that reacted with hyperimmune serum against Hendra virus by immunohistochemistry (IHC). All four specimens were negative for JE antigen. Laboratory studies at CDC and in Malaysia demonstrated Hendra-virus IgM antibodies in serum specimens of 23 (88%) of 26 cases; in addition, Hendra-like antigens were detected in central nervous system tissue from four of five case-patients and from lung and kidney tissues of one case-patient tested. Hendra-like virus sequences have been found in four case-patients. Central nervous system, lung, and kidney tissues from swine from affected farms in Malaysia also have been positive for Hendra-like antigens by IHC. Epidemiologic Features Illness has been characterized by 3-14 days of fever and headache followed by drowsiness and disorientation that can progress to coma within 24-48 hours; a few patients had respiratory illness. Of the 229 case-patients, most have been men working on pig farms in Perak and Negri Sembilan. One case-patient became ill 10 days after his last known exposure to swine. Five cases have been reported in Malaysian abattoir workers exposed to swine. No cases have been reported among health-care workers caring for case-patients. In some instances, illness in pigs occurred 1-2 weeks before illness in humans. The disease in swine is not well defined but appears to include rapid and labored breathing; an explosive nonproductive cough; and neurologic changes, including lethargy or aggressive behavior. Case Report On March 7, 1999, a 49-year-old pig farmer in Malaysia developed fever, headache, behavior changes, and mild blurred vision. The following day, he became lethargic and was subsequently hospitalized with a diagnosis of viral fever. During the next several days, the farmer's neurologic status progressively worsened, and he developed generalized seizures, respiratory failure requiring mechanical ventilation, blood pressure instability, and high spiking fevers. He died on March 13. On admission, complete blood count, electrolytes, and head computed tomography scan were normal. A lumbar puncture performed on March 13 showed no white blood cells, a normal glucose level, and a protein level of 2.09 g/L (normal: 0.15-0.45 g/L). The patient's serum was negative for JE virus IgM antibodies; his serum and cerebrospinal fluid (CSF) specimens were positive for Hendra-like virus IgM and IgG antibodies. A brother who had worked on the same pig farm and had died a few days earlier from encephalitis also had IgM antibodies to Hendra-like virus in both serum and CSF. SINGAPORE All 11 case-patients had handled swine imported from Malaysia. Serologic testing at CDC confirmed recent Hendra-like virus infection in these 11 workers, and limited nucleotide sequence studies of the virus from the patient who died suggest it is identical to that from the Malaysia outbreak. Antibodies to Hendra virus were detected at the Australian Animal Health Laboratories in blood samples from four of 100 pigs imported from Malaysia for slaughter in another Singapore abattoir. PUBLIC HEALTH ACTIONS In addition to active surveillance for encephalitis cases, studies are under way to determine risk, if any, for human-to-human transmission among health-care workers and family members, to confirm the source of human infection (presumedly pigs), to define specific risk factors associated with exposures to pigs and tissues from infected animals, and to determine the case-to-infection ratio and the epidemiology of this infection in pigs. Preliminary assessment suggests that spread of the virus among states in Malaysia has occurred through transport of infected swine. Susceptibility of other animal species is not known, and studies are under way to determine a presumed wildlife reservoir of this virus. To prevent further outbreaks, Malaysian authorities have banned transport of pigs within the country. Army personnel and police are enforcing this ban, and quarantined pigs are being culled within a 3-mile (5-km) perimeter around recognized outbreak areas. In addition, Malaysian authorities recommend that all persons in the affected areas who have exposure to pigs (e.g., farm workers, truck drivers transporting animals, abattoir workers, and soldiers assisting in quarantine and culling of swine) use protective equipment, including protective clothing, gloves, boots, and masks. Singapore and Thailand have banned importation of pigs from Malaysia. Singapore also has banned horses returning from Malaysia. The Malaysian MOH has initiated an education campaign to inform the public about the outbreak and about precautions during contact with pigs. Reported by: Dept of Medical Microbiology, Univ of Malaya, Kuala Lumpur; Institute for Medical Research; Vector Borne Disease Control Section, Disease Control Div, Ministry of Health; University Hospital, General Hospital, Kuala Lumpur; Seremban Hospital, Seremban; Ipoh Hospital, Ipoh; Institue of Veterinary Research, Veterinary Svc, Ministry of Agriculture; Ministry of Public Health, Malaysia. Changi General Hospital; Singapore General Hospital; Tan Tock Seng Hospital; Ministry of the Environment. Ministry of Health; Primary Production Dept, Ministry of National Development, Singapore. Commonwealth Scientific and Industrial Research Organization, Australian Animal Health Laboratory, Geelong, Queensland Dept of Primary Industries, Brisbane, Australia. Arbovirus Diseases Br, Div of Vectorborne Infectious Diseases; Div of Quarantine; Respiratory and Enteric Virus Br, Special Pathogens Br, Infectious Diseases Pathology Activity, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; and EIS officers, CDC. Editorial NoteEditorial Note: Hendra virus was first recognized in September 1994 after an outbreak of respiratory illness among 20 horses and two humans in Hendra, Queensland, Australia (1); 13 horses and one human died. In 1995, a second unrelated outbreak was identified that had occurred in August 1994 in Mackay, Queensland, in which two horses died and one human became infected (2,3). Transmissibility of Hendra virus from infected horses to other species appears to be low (4). All three previous human infections appear to have been acquired through exposure to blood or other body fluids or excretions of infected horses. Laboratory evidence suggests that fruit bats (Pteropus species) found in Australia (5) and in Papua New Guinea may be the natural host for the virus. Despite close contact between fruit bats and bat researchers in Australia, serologic evidence of infection has not been found in these persons (6). The previously unrecognized paramyxovirus associated with these outbreaks of febrile encephalitis in Malaysia and Singapore is related to, but distinct from, the Australian Hendra virus (7). Serologic and IHC analyses support a causative role for this new virus in human and swine disease. Studies are under way to clarify what proportion of these illnesses is caused by infection with Hendra-like virus. The association between the disease in humans and pigs is supported by epidemiologic and laboratory data. Although the specific routes of transmission have yet to be determined, close contact with pigs appears to be necessary for human infection. Travelers to Malaysia should be aware of these outbreaks of febrile encephalitis, which have involved only those closely associated with swine. No travel restrictions have been recommended or imposed at this time. U.S. residents anticipating travel to Malaysia should follow the CDC regional recommendations for Southeast Asia, which are available on the World-Wide Web at http://www.cdc.gov/travel/index.htm or http://www.cdc.gov/travel/seasia.htm. Persons in Malaysia are advised to contact the Malaysian health authorities for additional information. Information about the recent cases is available at the Malaysian Ministry of Health website at http://dph.gov.my. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 04/08/99 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}